
Workplace Testing Planner
Get answers to your most common COVID related questions.
For basic information on the disease and how to help reduce the spread, visit:
Tests & Testing
Screening for COVID-19, also referred to as screening testing or asymptomatic screening, means testing your population to identify infected people who are not showing symptoms. Diagnostic testing for COVID-19 is performed when infection is suspected, such as when the person:
Has COVID-19 symptoms or
Has no symptoms, but has had a recent known or suspected exposure to SARS-CoV-2 (the virus that causes COVID-19).
As of September 26, 2022, only tests that have Emergency Use Authorization (EUA) for use in asymptomatic people can be used for screening. To see which PCR tests can be used, go to this page of the FDA's website and search for "screening." To see which antigen tests can be used, go to this page of the FDA's website and search for "screening."
Both kinds of testing can be done using either a PCR test (also known as a molecular or lab test) or an antigen test (also called a rapid test).
PCR tests look for pieces of the virus’s genetic material. They are the most accurate kind of test for COVID-19 currently available.
Antigen tests look for proteins from the virus. They are designed to be taken at least twice: If you have COVID-19 symptoms, you take one test now, and one test 48 hours later. If you don't have symptoms, wait another 48 hours and take a third test. When used that way, they are nearly as accurate as PCR tests. If you're using antigen tests for screening, you'll need to test more frequently than you would if you were using PCR tests.
Antibody tests (also known as serology tests) look for proteins that your body makes to fight the virus. Those proteins are called antibodies. They can come from a past COVID-19 infection or from a COVID-19 vaccine. Antibody tests cannot be used to diagnose an active infection.
FDA – Coronavirus 2019 Test Basics
Confirmatory testing is done to make sure the results of a test are correct. Here are the situations in which it might be recommended:
When someone tests negative on an antigen test even though they have COVID-19 symptoms or were recently exposed to someone who has COVID-19.
When someone tests positive on a test with a specificity of less than 99%, especially when COVID-19 levels are low.
Asymptomatic screening programs are frequently supplemented by confirmatory testing because false positives are more common when screening asymptomatic individuals.
In point-of-care (POC) testing, all testing steps, including sampling and analysis, take place close to or near the patient. For the Workplace Testing Planner and the COVID Risk Quiz, this means that testing is completed either on-site at your organization’s location or in a health-care provider's office, at a testing site, or in your home. Point-of-care tests give you results quickly. Most of them are antigen tests, but some point-of-care PCR tests are available, as well.
In lab-based or off-site testing, samples are gathered on-site at your organization or other testing location and are sent to a central lab for processing and analysis. Lab-based tests are generally PCR tests, which are highly accurate. However, they take longer to return results than point-of-care tests do. In some cases, the turnaround time of lab-based tests is not fast enough to prevent an outbreak in an organization.
CDC – Guidance for SARS-CoV-2 Point-of-Care and Rapid Testing
Sensitivity refers to how well a test designates someone who HAS the disease as positive.
If you have a test with 95% sensitivity and you test 100 people who have COVID-19, 95 will test positive (true positive) and 5 will test negative (false negative). Tests with high sensitivity will find most cases of the virus. They will return few false negatives.
Specificity is how well a test designates someone who DOESN’T have the disease as negative.
If you have a test with 95% specificity and you test 100 people without COVID-19, 95 will test negative (true negative) and 5 will test positive (false positive). People who test positive using tests with high specificity are very likely to truly have the disease, which means that very few people will be quarantined unnecessarily. These tests return few false positives.
In an ideal world, all tests would be both highly sensitive and highly specific. Unfortunately, that’s not possible most of the time. It’s also important to acknowledge that no test is perfect — no test will have 100% sensitivity and specificity.
When you're using a test to find out if someone has a disease, there are four possible results you can get:
True positive: The test result is positive and the person has the disease.
True negative: The test result is negative and the person doesn't have the disease.
False positive: The test result is positive but the person doesn't have the disease.
False negative: The test result is negative but the person does have the disease.
In an ideal world, all tests would return only true positives and true negatives. Unfortunately, no test is perfect.
Pooled testing, also known as pooling, is a way to make highly sensitive PCR testing more cost-effective. In pooled testing, samples are gathered from multiple people and mixed together into a pool. Instead of testing each individual sample on its own, the lab tests the pool, thus using fewer resources and lowering processing costs.
If a pool tests negative, then all individuals in that pool are ‘clear’ or negative for COVID-19 and may continue to attend class, work, or other activities.
If a pool tests positive, then at least one individual in the pool may be positive for COVID-19. When this happens, follow-up testing, sometimes referred to as “reflex testing” or “deconvolution,” is required. Follow-up testing can be done at a central lab or on-site.
In follow-up testing, each person or each sample in the positive pool is individually retested to determine which individual(s) in the positive pool are infected. If follow-up testing isn’t possible, then the entire pool should isolate. Pooled testing should be done at a lab, using a PCR test that has Emergency Use Authorization (EUA) from the FDA. The lab’s pooling system should either have EUA or be internally validated.
CDC — Interim Guidance for Use of Pooling Procedures in SARS-CoV-2 Testing
FDA — Pooled Sample Testing and Screening Testing for COVID-19
Open and Safe Schools — Includes toolkit on how to start a pooled testing program at your school.
Follow-up testing is a critical part of pooled testing. In pooled testing, samples are gathered from multiple people and mixed together into a pool. Instead of testing each individual sample on its own, the lab tests the pool. If a pool tests positive, then at least one individual in the pool may be positive for COVID-19. When this happens, follow-up testing, sometimes referred to as “reflex testing” or “deconvolution,” is required. If follow-up testing isn’t possible, then the entire pool should isolate.
In follow-up testing, each person or each sample in the positive pool is individually retested to determine which individual(s) in the positive pool are infected. The way follow-up testing happens depends in part on how and where the samples are pooled.
The Workplace Testing Planner identifies four testing strategies for follow-up testing a positive pool. Details on each strategy appear beneath the table below.

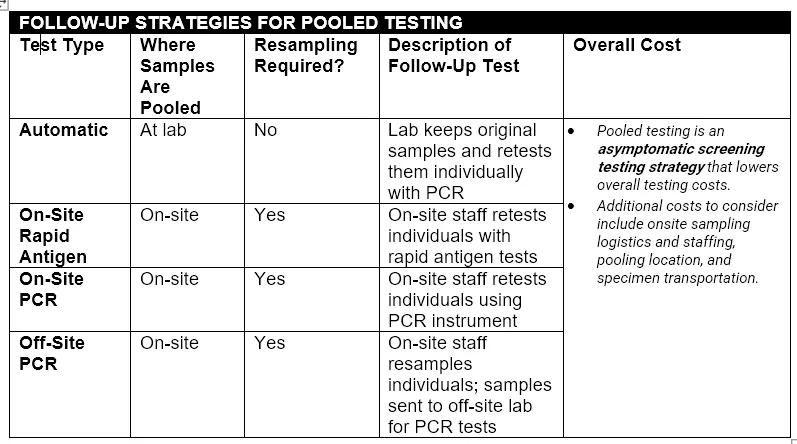
AUTOMATIC
Pooling Process: Individual samples are collected on-site and taken to an off-site lab. The lab creates the pools and tests the pooled samples using PCR.
Follow-Up Testing Process: When a positive pool is identified, the lab automatically retests the individual samples that went into the pool using PCR.
Pros and Cons
Eliminates need to re-collect individual samples.
Results are provided faster than other pooled testing strategies.
May be 2-3x more costly per test than rapid antigen and on-site PCR follow-up.
ON-SITE RAPID ANTIGEN
Pooling Process: Individual samples are collected and pooled on-site. The pooled samples are taken to an off-site lab, which tests them using PCR.
Follow-Up Testing Process: When a positive pool is identified, all individuals in the positive pool must be resampled. Individual follow-up tests are completed on-site, using rapid antigen tests.
Pros and Cons
Faster than off-site PCR follow-up.
Likely to be least expensive option.
Requires trained staff on site.
Slightly less accurate than PCR follow-up, because antigen tests aren't designed to be used this way. They're supposed to be used twice: You take one test now, and one a day or two later.
ON-SITE PCR
Pooling Process: Individual samples are collected and pooled on-site. The pooled samples are taken to an off-site lab, which tests them using PCR.
Follow-Up Testing Process: When a positive pool is identified, all individuals in the positive pool must be resampled. Individual follow-up tests are completed on-site, using PCR instruments.
Pros and Cons
Faster than off-site PCR follow-up.
Less expensive than automatic or off-site PCR follow-up.
Requires PCR instruments and trained staff on site.
Highly accurate.
OFF-SITE PCR
Pooling Process: Individual samples are collected and pooled on-site. The pooled samples are taken to an off-site lab, which tests them using PCR.
Follow-Up Testing Process: When a positive pool is identified, all individuals in the positive pool must be resampled. Samples are shipped to an off-site lab, where individual follow-up tests are completed with PCR.
Pros and Cons
Slowest pooling option.
More expensive than on-site follow-up.
Highly accurate.
Pooled testing, also known as pooling, is a way to provide highly sensitive PCR testing for your organization in a more cost-effective way. In pooled testing, samples are gathered from multiple people and mixed together into a pool. Instead of testing each individual sample on its own, the lab tests the pool, thus using fewer resources and lowering processing costs.
Pooled testing could be a good fit for your organization if:
Positivity rates in your community are relatively low (i.e., you don’t expect a lot of people in your organization to test positive).
You want the sensitivity of PCR testing.
You don’t want to train or pay staff to do testing on-site (however, some types of pooled testing do require on-site follow-up testing).
You can’t test more frequently than once a week.
Pooled testing is not a good fit for your organization if:
Positivity rates in your community are very high (i.e., you expect a lot of people in your organization to test positive).
You need immediate test results.
CDC — Interim Guidance for Use of Pooling Procedures in SARS-CoV-2 Diagnostic and Screening Testing
FDA — Pooled Sample Testing and Screening Testing for COVID-19
Open and Safe Schools — Includes toolkit on how to start a pooled testing program at your school.
PCR tests, also known as molecular tests, look for pieces of the virus’s genetic material using a lab technique called polymerase chain reaction (PCR). They are the most accurate kind of test for COVID-19 currently available.
PCR samples are usually sent for processing and analysis in a lab, and results can take anywhere from a few hours to several days to arrive. Lab-based PCR tests tend to cost more than other test types. Some point-of-care PCR tests are now available, but they typically require purchase of a dedicated instrument and training to run the tests. If you want to use a point-of-care PCR test to screen members of an organization, you may need to purchase multiple instruments and train several staff members for this purpose. Point-of-care PCR tests typically return results in under an hour.
Antigen tests look for viral proteins. These tests typically provide results within minutes and are very good at accurately identifying people who are carrying a lot of virus. They are not as good as PCR tests at finding people who aren't carrying as much virus, including children and asymptomatic adults. If your organization is using this type of test, check how well the brand you use works in the population you’ll be testing (adults vs. children, people with symptoms vs. people without symptoms). Many antigen tests still require trained staff run them, but others are now available over the counter for home use. Antigen tests tend to be the least expensive type of test.
Because of their decreased sensitivity, antigen tests have the following limitations:
If you are using antigen tests to screen members of an organization, you may need to test more frequently than you would if you were using a PCR test in order to prevent an outbreak.
If you have symptoms or were recently around someone with COVID, a positive result on an antigen test is usually correct, but a negative test result might not be right. If you just got infected, you may not have enough virus in your system for a rapid test to detect.
Once your virus levels have gone up, a rapid test will show a positive result.
If you have symptoms, it's best to take a second test 48 hours after the first. If you were exposed but don't have symptoms and test negative on both of those tests, it's best to take a third test 48 hours later.You can also get a lab test to confirm your result.
Be sure to follow all of the instructions that came with the test.
Remember, no test is perfect.
In addition to the cost of the individual test kits, take a look at the following:
Accuracy: Most antigen tests have a very high specificity. However, the sensitivity of the different brands of tests varies. (The Workplace Testing Planner assumes a lower sensitivity for antigen tests than with PCR tests, to ensure that the recommended testing frequency is adequate to prevent an outbreak.)
Capital expenditures and maintenance: Some antigen tests run on a small testing instrument, which must be purchased separately and maintained over time. Depending on size of your organization, you may need to purchase several of these instruments in order to be able to test your population quickly enough to prevent an outbreak.
Staffing requirements: Some antigen tests require trained staff to obtain samples and/or run the tests. If you use an instrument-based antigen test, you will need staff to maintain the instruments, as well. Other types of antigen tests can be performed entirely by the person being tested.
Time: Some rapid antigen tests can be done at home, decreasing the amount of time taken away from work or school for testing purposes.
Access: Manufacturing of antigen tests has not always kept up well with demand, so some businesses may find they have a limited selection of brands from which to purchase. Some schools will only have access to a single type of antigen test, which is provided or mandated by the state.
If they’ve been kept dry and at room temperature, they’ll probably still work, especially if they expired only recently. In fact, they may not be expired at all.
The expiration dates of most rapid tests have been extended by the FDA. To find out whether your rapid test's expiration date has been changed, go to the FDA's website and look for the brand of test you have. If you see the word "extended" in the Expiration Date column, then the FDA has changed the expiration dates. Click on the link in that column.
When you get to the next screen, look in the left or middle column for the expiration date that’s printed on the box you have. The date in the right-hand column is the new expiration date for your test.
If you live in California, your state department of public health has decided that you can use your test no matter what the date on the box says, as long as the control line appears when it’s supposed to.
On-site PCR tests use a small instrument to conduct a polymerase chain reaction (PCR)-based test on a sample. Depending on the size of your organization, you may need to purchase multiple instruments in order to test your population quickly enough to prevent an outbreak.
On-site PCR tests are not quite as sensitive as in-lab PCR tests, but they are typically more sensitive than antigen tests. These tests return results quickly – typically in under an hour – but are not as fast as rapid antigen tests. They require trained staff to run and maintain them.
If your organization is running tests in a central lab that you own (for example, a university lab), you should model your situation using off-site PCR tests.
The best way to avoid false positives is to choose a test with high specificity (>99%). A test’s specificity indicates how good it is at designating someone who DOESN’T have the disease as negative. People who test positive using tests with high specificity are very likely to truly have the disease, which means that very few people will be isolated and quarantined unnecessarily.
If you’re in an area with very low prevalence of disease, it’s especially important to choose a test with high specificity, because the likelihood of false positives becomes higher under those conditions.
Antibody tests (also known as serology tests) can't tell you if you have COVID right now. All they can tell you is whether you've had COVID or been vaccinated for COVID in the past.
Antibodies are proteins made by your immune system to help you fight off things like viruses and bacteria. When you get infected with a virus, your body makes antibodies that recognize and attach to that specific virus. It can take up to three weeks after the infection for your immune system to make enough antibodies to detect with a test.


The Food and Drug Administration (FDA) decides which drugs and medical tests can be used in this country. The full FDA approval process can take months to years.
When a public-health emergency happens, there isn’t time for new drugs or tests to go through the entire process. That’s when the FDA can use Emergency Use Authorization (EUA). It allows the FDA to let certain medical products be used more quickly, while still making sure they are as safe as possible. At a minimum, the product must have known and potential benefits that outweigh its known potential risks. In addition, there must be “no adequate, approved, and available alternatives” to the product receiving the EUA.
All treatments and tests for COVID used in the US have received an EUA - none of them have gone through the full approval process yet. The Pfizer and Moderna vaccines have received full approval from the FDA for adults. The Pfizer vaccine has an EUA for children ages 11 to 16.
Variants are mutated forms of SARS-CoV-2, the virus that causes the disease COVID-19. The variants that cause concern are ones whose mutations make them more likely to spread from person to person, cause more severe disease, and/or are able to more easily infect people who have been vaccinated.
All COVID-19 tests that have Emergency Use Authorization (EUA) from the FDA must be checked on an ongoing basis to make sure that they are able to detect different variants of the virus. If a test has any difficulty detecting a variant, the FDA must be notified immediately.
NOTE: As part of its calculations, the Workplace Testing Planner includes a default measurement of how transmissible the virus is. That measurement is called R0 (“R-naught”) or the basic reproduction number for the virus. WhenToTest.org follows CDC guidance to set the Planner's default for R0. If you would like to set a specific R0 in your scenarios, you can do so under Advanced Settings: Main Planner Settings.
CDC — What You Need to Know About Variants
R0 (R-naught) is a measure of the average number of people who will contract a contagious disease from one infected person. It’s a measure of viral transmissibility, or how fast the disease is spreading.
When R0 is exactly 1.0, it means that, on average, one infected person will infect one other person. When R0 is less than 1.0, it means that the spread of the disease is decreasing within the community. When R0 is above 1.0, the spread of disease is increasing. The more transmissible a disease or disease variant is, the higher its R0.
CDC — COVID Data Tracker, Variant Proportions
World Health Organization — Tracking SARS-CoV-2 Variants
Johns Hopkins Medicine — COVID Variants - What You Should Know
Prevalence is the percentage of people in a population who have a disease. So if there are 100 people in your area and 10 of them have COVID-19, the prevalence of COVID-19 in your area is 10%.
Technically, the only way to determine the true prevalence of COVID-19 in a population is to test every single person in the population to see who has it and who doesn't. Since that's not feasible, the Workplace Testing Planner and the COVID Risk Quiz use a sophisticated machine-learning model that looks at all of the available COVID-19 data for a particular state and county and develops a "predicted prevalence" for that location.
For US territories and areas outside the US, the Planner and the Quiz use a prevalence of 1% for typical conditions, and 3% for hotspot conditions.
Both the Workplace Testing Planner and the COVID Risk Quiz are based on CDC guidelines. Current guidelines define a “close contact” as someone who was within six feet of an infected person for a total of at least 15 minutes over the course of 24 hours. One exception to that rule is applicable only to schools: Students who were between three and six feet of an infected person are not considered close contacts as long as they were in school and “correctly and consistently” wearing masks.
COVID-19 Prevention
The more people in your organization who are vaccinated, the less testing you will need to do to prevent an outbreak. If most people in your organization have received booster shots, you will need to do even less testing. If you aren’t sure what percentage of your organization has been fully vaccinated or has received at least one booster, you can use published estimates for your area, available via the links below.
If you plan to test only the unvaccinated members of your organization, then the number you enter for the "Fully Vaccinated" input should be zero. Please note: The CDC recommends that when screening testing is used, it should include all members of a population, whether they're vaccinated or not.
CDC — COVID Data Tracker, COVID-19 Vaccinations in the United States - State-by-state vaccination statistics.
Yes. The Planner uses an estimate of how well the vaccines available in the US protect against the variant that is currently dominant in the country. This estimate is based on the performance of all available vaccines, not on any one vaccine brand or type.
If you are using the Workplace Testing Planner and want to adjust the Planner's default so that it matches a specific vaccine, go to the Advanced Settings, click on "Main Planner Settings," and look for "Vaccine Effectiveness."
Yes, but people may choose on an individual basis to decline to answer the question. Once an employer has information about an individual’s vaccine status, they must keep it confidential and separate from the rest of the employee’s personnel files, per the Americans with Disabilities Act (ADA).
US Department of Health and Human Services – The HIPAA Privacy Rule
US Equal Employment Opportunity Commission – Coronavirus and COVID-19
For information about this and other questions about COVID-19 regulations in the workplace, please check the US Equal Employment Opportunity Commission’s (EEOC) website, listed below.
Vaccination requirements for students are typically set at the state level. Please contact your state department of education for further guidance.
US Equal Employment Opportunity Commission – Coronavirus and COVID-19
The more people in your organization who wear masks consistently and properly, the less testing you will need to do to prevent an outbreak. Remember: a well-fitted mask, worn properly, covers both the nose and the mouth and does not leave gaps. The Workplace Testing Planner asks you to estimate what percentage of people in your organization wear their masks properly at all times when indoors. Most people tend to overestimate the percentage of people in their own organizations who do this, so you may want to input a number a bit lower than you were first considering.
The type of mask people wear also matters. Two-layer cloth masks have a filtration efficiency of about 30%. For surgical masks that fit well, without gaps, that number is about 70%. For KN95 masks, it’s about 85%. If everyone at your organization wears high-efficiency masks, your testing needs will decrease.
Find high-quality masks at Project N95.
The faster your organization can identify and notify close contacts of an infected person, the lower your need for testing will be. The reason for this has to do with how contact tracing works and how it affects the likelihood of an outbreak.
The goal of contact tracing is to identify the people who were in close contact with an infected person while they were contagious, so that those people can be prevented from spreading the disease to others. The faster close contacts are identified and notified of their status, the sooner they can quarantine, and the less likely it is that they will infect other people.
For COVID-19, the definition of a close contact is someone who was within six feet of an infected person while they were contagious, for a total of at least 15 minutes over the course of 24 hours. (One exception to that rule is applicable only to schools: Students who were between three and six feet of an infected person are not considered close contacts as long as they were in school and “correctly and consistently” wearing masks.) When someone with no symptoms tests positive for COVID-19, it’s assumed that they were contagious for the 48 hours (two days) before they provided the sample that was tested.
In practice, identifying exactly who has been in “close contact” with someone over the course of two days can be quite difficult unless your organization keeps good records. Schools often keep seating charts for classrooms, school buses, and lunch tables for this purpose. In addition, teachers may keep track of which students tend to walk next to one another in the hallways. In an office setting, keeping records of in-person meeting attendance and assembly-line stations may be helpful.
NOTE: The Workplace Testing Planner assumes that only 50% of an infected person’s close contacts are identified and notified of their status within 24 hours (a contact-tracing efficiency of 0.5). This assumption may be changed in the Planner's defaults under Advanced Settings: Main Planner Settings.
Limiting the size of groups who participate in these kinds of activities together indoors and unmasked is an extremely effective way to reduce COVID-19 transmission risk, and thus reduce your organization’s need for testing.
With increasing levels of vaccination in the US, many organizations have decided to do away with mask-wearing altogether. However, some activities remain higher risk than others in terms of their potential for COVID transmission. Any activity that brings a group of people together in close proximity for an extended period of time – most commonly, eating and/or drinking together at the same table – carries a high risk. Other high-COVID-risk activities are those that involve breathing heavily and/or with force, such as sports activities, singing, and playing wind instruments, whether or not the participants are in close proximity to one another.
If your organization permits either of these types of activities indoors, then the number you would input in this section of the Workplace Testing Planner is the largest group that participates in such activities together. For example, if you have a choir of 10 people and a basketball team of 25, you would input “25.” Doing so allows the Planner to factor in the additional layer of risk added by permitting these kinds of activities to happen indoors.
NOTE: The Planner assumes that cohorts of people eating or drinking together are physically distanced from other people in the room. Thus, if your cafeteria has 20 tables that each seat a cohort of eight people and the tables are more than six feet apart, the size of the cohort is eight.
However, physical distancing has its limits. If people in your organization are participating in unmasked indoor group activities that involve significant exertion or air expulsion (for example, sports, gym classes, or singing), then the cohort size should be the total number of people in the room, regardless of their distance from one another.
For COVID-19, the definition of a close contact is someone who was within six feet of an infected person while they were contagious, for a total of at least 15 minutes over the course of 24 hours. (One exception to that rule is applicable only to schools: Students who were between three and six feet of an infected person are not considered close contacts as long as they were in school and “correctly and consistently” wearing masks.) When someone with no symptoms tests positive for COVID-19, it’s assumed that they were contagious for the 48 hours (two days) before they provided the sample that was tested.
In practice, identifying exactly who has been in "close contact" with someone over the course of two days can be quite difficult unless your organization keeps good records. Schools often keep seating charts for classrooms, school buses, and lunch tables for this purpose. In addition, teachers may keep track of which students tend to walk next to one another in the hallways. In an office setting, keeping records of in-person meeting attendance and assembly-line stations may be helpful.
NOTE: The Workplace Testing Planner assumes that only 50% of an infected person’s close contacts are identified and notified of their status within 24 hours (a contact-tracing efficiency of 0.5). This assumption may be changed in the Planner's defaults under Advanced Settings: Main Planner Settings.
Using the Planner
The Planner and the Quiz have different goals and base their recommendations on different inputs.
The goal of the COVID Risk Quiz is to estimate your risk of having or getting COVID-19. It does that by taking information about how COVID-19 is behaving these days and combining that with information about your activities and your personal COVID-19 history. (This Quiz is a decision-support tool only. Results are provided for informational purposes and should not be construed as medical advice.)
The goal of the Workplace Testing Planner is to decrease the overall risk of an outbreak within a workplace or school. It does that by evaluating the COVID mitigation strategies in place at the organization and recommending the appropriate level of testing needed to complement those strategies.
You are in a COVID-19 hotspot if:
There have been at least 100 cases of COVID-19 per 100,000 people in your area over the past seven days, and/or
The test positivity rate in your area is currently 10% or higher.
The number of cases per 100,000 people is called the incidence rate. If you are outside the United States, you can find your country's seven-day incidence rate here.
If you are in a US territory other than Puerto Rico, you can find your territory's incidence rate on this map in the CDC's COVID Data Tracker. Puerto Rico is on the drop-down list of US states in the Planner itself.
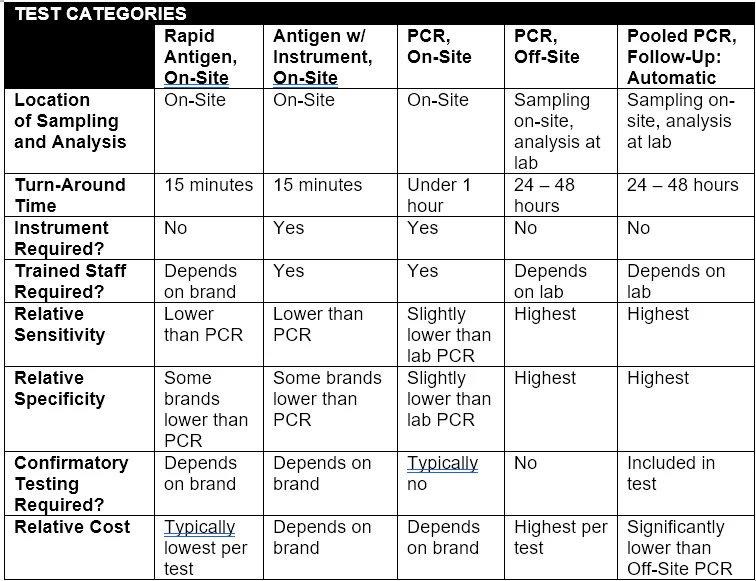
Both Rapid Antigen tests and Antigen w/ Instrument tests are point-of-care COVID-19 tests that look for viral proteins and return results within minutes. For the purposes of this Planner, the differences between these two types are as follows:
Rapid Antigen Test
Looks like a pregnancy test
Once the test is used, it is thrown out
Some of these tests can be completed by the person being tested; others require trained staff to obtain samples and/or run the test itself
Has a lower sensitivity than Antigen w/ Instrument (see note below)
Antigen w/ Instrument
Requires a small piece of equipment to run the test
The instrument must be purchased separately from test kits and maintained over time
Your organization may need to purchase several instruments in order to be able to test your population quickly enough
Requires trained staff to run the tests and maintain the instrument(s)
Has a higher sensitivity than Rapid Antigen (see note below)
There may be additional considerations for a workplace to consider one antigen test over another.
IMPORTANT NOTE: The sensitivity and specificity of both Rapid Antigen tests and Antigen with Instrument tests vary a great deal between test brands. If your organization decides to use one of these test types either for asymptomatic screening or for follow-up for pooled testing, check the sensitivity and specificity of the brand of test you plan to use. Then go to Advanced Settings in the Planner, click on the tab for the relevant test type, and adjust the sensitivity and specificity settings to match your brand of test.
The Planner is designed so that you can compare how your organization’s testing needs would change if you altered your mitigation strategies. It can also allow you to compare the testing needs of different cohorts of people within your organization.
The amount of testing your organization needs to do depends in part on the type of test you use. This Calculator returns results for the test categories listed in the table below, as well as additional results for other pooled testing strategies. NOTE: The test categories shown in the Calculator are examples only; they do not represent any one individual test.

For more information, see the following FAQ topics:
What’s the difference between PCR and antigen tests?
What's the difference between a Rapid Antigen Test and Antigen w/ Instrument in the Calculator?
In general, antigen tests are less sensitive than PCR tests. That means they are not as good as PCR tests at finding people who aren't carrying as much virus, including children and asymptomatic adults. Testing more frequently helps to make up for the antigen tests’ lower sensitivity. Most rapid tests are designed to be used at least twice: You take one test now and one test 48 hours later. If you don't have COVID-19 symptoms and test negative on both of those tests, you take a third test 48 hours after the second one. If you use them that way, you'll get the most accurate result.
In addition, people who were infected very recently often carry low levels of virus, so if you test them using an antigen test at that time, they may test negative. Once their virus levels have risen significantly (from a few hours to a day or two later), an antigen test will come back positive. Because PCR is more sensitive, it can catch an infection early in the disease course, eliminating the need for another test.
The Workplace Testing Planner tells you how often your school or workplace needs to perform what is called “asymptomatic screening,” or testing people who do not have COVID-19 symptoms. The goal of asymptomatic screening is to find and isolate infected people who do not have symptoms, in order to prevent them from transmitting the virus to others.
If your conditions are favorable and your organization has excellent mitigation measures in place, you may not need to do asymptomatic screening in order to effectively reduce the chance of an outbreak. In those cases, the Planner will recommend “Symptomatic Screening Only,” meaning that you should continue to require COVID-19 testing for people who display symptoms, but you do not need to test those who are symptom-free.
NOTE: The Planner's results are based upon the CDC’s most recent guidance regarding how transmissible the most common variants of the virus are. It’s a good idea to be prepared to institute asymptomatic screening should your organization’s situation change, and to frequently recheck the Planner's results for your organization.
The Planner is designed to assess only your organization's need for asymptomatic screening: regular, ongoing testing of individuals who do not have symptoms of COVID-19. If your organization does not need asymptomatic screening, then no resources or staff for that type of screening are required.
There are three main reasons why you might get that result.
Your mitigation strategies aren't strong enough.
Your organization doesn't offer testing on enough days of the week.
Regardless of the reason why you received the warning message, improving mitigation strategies is the best way to lower your organization's risk of an outbreak. You can make those improvements by doing any (or all) of the following:
Incentivizing or requiring vaccination and booster shots.
Encouraging or requiring everyone to wear high-quality masks properly and consistently.
Keeping better track of close contacts.
Decreasing the size of cohorts that participate in unmasked activity together.
Testing can only help prevent an outbreak if your organization receives test results in time to isolate infected people and quarantine their close contacts before they can spread the virus. In some situations, the amount of time it takes Off-Site PCR and Pooled PCR results to come back will be too long, based on the Planner's default settings.
If turnaround time is your problem, then you may be able to work with your lab to fix it. The Planner assumes that it takes 36 hours to receive test results from an off-site lab. If your lab can return results in less time, go to Advanced Settings and click on the tab for the type of test you've chosen. Then scroll down to "Lab turnaround time, in hours" and change the default there.
And remember, even if the Planner is giving you this result, improving your mitigation strategies is likely to help you to decrease the likelihood of an outbreak, as well.
The Planner assumes that people in your organization are on-site and can be tested five days a week. If you get this result, it means that people would need to be available for testing more than five days a week in order to reduce the chance of an outbreak. (Note: For the purposes of this result, the Planner also assumes that testing is spread out over the course of a week, and different individuals in your organization get tested on different days.)
If testing takes place at your organization seven days a week, go to Advanced Settings, click on the Main Planner Settings tab, and change the setting on "Days per week that testing is done?" to "7."
Note that in some situations, even daily testing will be inadequate; in those cases, you may need to improve your mitigation strategies in order to decrease the risk of an outbreak. And remember, even if switching to daily testing does solve the problem, improving your mitigation strategies may help outbreaks become even less likely.
If you see this result, you will need to improve your organization's COVID-19 mitigation measures other than testing in order to help decrease the risk of an outbreak; adding testing alone will not be enough.
Regardless of the reason why you received the warning message, improving mitigation strategies is the best way to lower both your organization's reliance on testing and its risk of experiencing an outbreak. You can make those improvements by doing any (or all) of the following:
Incentivizing or requiring vaccination and booster shots.
Encouraging or requiring everyone to wear high-quality masks properly and consistently.
Keeping better track of close contacts.
Decreasing the size of cohorts that participate in unmasked activity together.
Use the Planner to model various scenarios and predict how improvements in these areas can change your test recommendations.
Some people in your organization may not be on-site every day. Those people still need to be tested on essentially the same schedule as those who are on-site on a daily basis.
For example, if the Planner lists the recommended max days between tests/person as “7,” then all individuals in your organization should be tested once every seven calendar days, regardless of how frequently they come to your site.
This calculation assumes that testing is uniformly spread across the testing period for onsite testing. If it is desired to complete all testing within a shorter period of time, then it may be necessary to hire more staff to conduct sampling and testing and to purchase additional instruments (if an instrument-based test is chosen).
Yes. You can use the Planner to evaluate the testing needs of your staff. When you input the size of your organization, do not include your clients or other visitors, only the members of your organization.
The Planner was developed as part of Project Isolat at MIT’s Institute for Data, Systems, and Society at MIT (IDSS). The article Simple Control for Complex Pandemics presents the model in detail.
This short video explains how the Planner was developed.
Testing Program Tips
The COVID-19 Testing Implementation Guide
This guide provides practical guidance on the implementation of a COVID-19 testing program, including consideration of various supply, personnel, facilities, and documentation best practices.
This website, created by the Shah Family Foundation in partnership with the CDC, provides schools and early education centers with the tools to create a comprehensive COVID-19 testing program. It also includes a list of vendors as well as a database of contacts at schools willing to share their experiences with COVID-19 testing.
Chiefs for Change Project Planning Workbook for K-12 COVID-19 Testing
This downloadable Excel spreadsheet, created by the educational leadership group Chiefs for Change, guides administrators step-by-step through the process of designing, implementing, and managing testing in a school district.
Visit our collaborator, Project N95, to find a number of COVID-19 tests available for purchase.
Connect to Test — Created by Arizona State University, this site allows users to input a series of criteria and receive a list of companies and test kits that meet those needs.
School COVID-19 Testing Partner List — Open and Safe Schools, created by the Shah Family Foundation in partnership with the CDC, provides a list of test vendors that are prepared to work with schools and early education centers. The list is searchable by state and by type of test offered.
Most of the COVID-19 tests on the market that have Emergency Use Authorization (EUA) from the FDA have received that authorization for diagnostic testing: testing individuals who have COVID-19 symptoms. Fewer tests have EUA specifically for screening: testing people who don’t have symptoms of COVID-19.
However, as long as the tests are used under the supervision of a physician or other prescriber, the FDA supports doing off-label screening testing with COVID-19 tests that only have EUA for diagnostic testing.
NOTE: The Workplace Testing Planner assumes that tests that do not have FDA authorization for screening are used off-label under practitioner guidance.
First, figure out what kind of test you are or will be using. (If you’re using pooled testing, you’ll also need to check what kind of follow-up testing you are or will be doing.)
You can find the list of test types for which the Planner provides results under the FAQ topic “What are the main differences between the various test types listed in the Planner's results?” If you’re not sure which type of test you are or will be using, check with your test vendor for confirmation.
Once you know your organization’s type of test, look at your results in the Planner and find the row that matches your test type. (If you’re using pooled testing, you may need to click on “View More Pooling Options” to find the type of follow-up testing your program is or will be using.) The results on that row are the Planner's recommended test frequency for your organization.
If the Planner's recommendations for your test type aren’t feasible for your organization, or if they indicate that you cannot prevent an outbreak using that type of test, consider how your organization might improve mitigation measures other than testing. You can make those improvements by doing any (or all) of the following:
Incentivizing or requiring vaccination and booster shots.
Encouraging or requiring everyone to wear high-quality masks properly and consistently.
Keeping better track of close contacts.
Decreasing the size of cohorts that participate in unmasked activity together.
Use the Planner to model various scenarios and predict how improvements in these areas can change your test recommendations.
If the Planner's recommendations for your test type aren’t feasible for your organization, or if they indicate that you cannot prevent an outbreak using that type of test, consider how your organization might improve mitigation measures other than testing. You can make those improvements by doing any (or all) of the following:
Incentivizing or requiring vaccination and booster shots.
Encouraging or requiring everyone to wear high-quality masks properly and consistently.
Keeping better track of close contacts.
Decreasing the size of cohorts that participate in unmasked activity together.
Use the Planner to model various scenarios and predict how improvements in these areas can change your test recommendations.
As their website states, “The Centers for Medicare & Medicaid Services (CMS) regulates all laboratory testing (except research) performed on humans in the US through the Clinical Laboratory Improvement Amendments (CLIA). . . The objective of the CLIA program is to ensure quality laboratory testing.”
Normally, labs need CLIA certification from CMS in order to perform testing. However, the FDA allows some tests to be performed at locations that do not have CLIA certification, as long as those sites have a CLIA waiver.
Your organization can apply for a CLIA waiver via the CMS CLIA website or your local State Agency.
It depends on who is gathering the samples and reading the results of the tests.
Your organization does NOT need a CLIA waiver if:
Adults being tested are swabbing themselves or providing saliva samples AND reading the results of their own tests.
Children are swabbing themselves or being swabbed by their parents/guardians, AND the parent/guardian is reading the results of their children's tests.
Adults who are unable to swab themselves are being swabbed by another adult.
Your organization DOES need a CLIA waiver if:
Adults who are able to swab themselves are being swabbed by someone else.
Adults swab themselves, and another person looks at the test result and decides whether it's negative or positive.
Children are being swabbed by an adult other than a parent/guardian.
Children are swabbing themselves, and someone who is not the children's parent/guardian looks at the test result and decides whether it's negative or positive.
For further details, see the links below.
CMS — Over The Counter (OTC) Home Testing and CLIA Applicability
CDC — Guidance for SARS-CoV-2 Rapid Testing Performed in Point-of-Care Settings
All PCR test results and all positive antigen test results for COVID-19 must be reported to public-health authorities. Negative antigen test results do not need to be reported. Reporting requirements can be found on the US Department of Health and Human Services website.
The confidentiality of COVID-19 test results is governed by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). If your organization is a school and is testing students, their test results are also likely to be governed under the Family Educational Rights and Privacy Act (FERPA).
US Department of Health and Human Services — HIPAA and COVID-19
When an individual in your testing program receives a positive result:
Isolate the individual as soon as possible.
Review test specificity, and if necessary, perform a confirmatory test.
If the person is a minor, contact their family or guardian.
Notify your local health department.
Notify the doctor or nurse practitioner who provided the standing order for your tests.
Initiate contact tracing.
When a pooled test sample comes back positive, all individuals in the positive pool should be isolated until follow-up testing can be performed. Once individual follow-up test results have identified the COVID-19 positive individual(s) in the pool, follow the protocol listed above.
If your conditions are favorable and your organization has excellent mitigation measures in place, you may not need to regularly test people without COVID-19 symptoms in order to effectively reduce the chance of an outbreak. In those cases, the Planner will recommend “Symptomatic Screening Only,” meaning that you should continue to require COVID-19 testing for people who display symptoms, but you do not need to test those who are symptom-free.
To reach this goal, consider how your organization might improve mitigation measures other than testing. You can make those improvements by doing any (or all) of the following:
Incentivizing or requiring vaccination and booster shots.
Encouraging or requiring everyone to wear high-quality masks properly and consistently.
Keeping better track of close contacts.
Decreasing the size of cohorts that participate in unmasked activity together.
Use the Planner to model various scenarios and predict how improvements in these areas can change your test recommendations.
Once you’ve modeled a scenario that you believe is achievable, take steps to make those improvements a reality within your environment.
NOTE: The Workplace Testing Planner's results for typical conditions are based upon the CDC’s estimate of R0 for the variant that is currently most common in the US, and upon the assumption that your organization has already performed baseline testing (testing 100% of all of its members prior to beginning an asymptomatic screening program). It’s a good idea to be prepared to institute asymptomatic screening should your organization’s situation change, and to frequently recheck the Planner's results for your organization.